



COVID-19 has dominated the global discourse for viral disease. However, a group of researchers based in Europe found a new variant of the human immunodeficiency virus (HIV). Called HIV-B, this variant has so far infected 17 patients participating in the BEEHIVE study1: 15 in the Netherlands, 1 in Switzerland, and 1 in Belgium. The BEEHIVE study investigates what genes in HIV make AIDS worse for patients. The patients enrolled in BEEHIVE are also part of a larger study – ATHENA – that examines HIV patient care in the Netherlands2. Within the ATHENA cohort, the authors found the variant in 96 of 6706 patients. Looking at those numbers, the new variant has likely not made its way to many HIV patients yet. Despite this, the variant has made headlines. That’s because patients infected by HIV-B experience worse disease than other HIV patients. To understand why the variant is so dangerous, we first need to understand how HIV infections work.
The nature of HIV infections
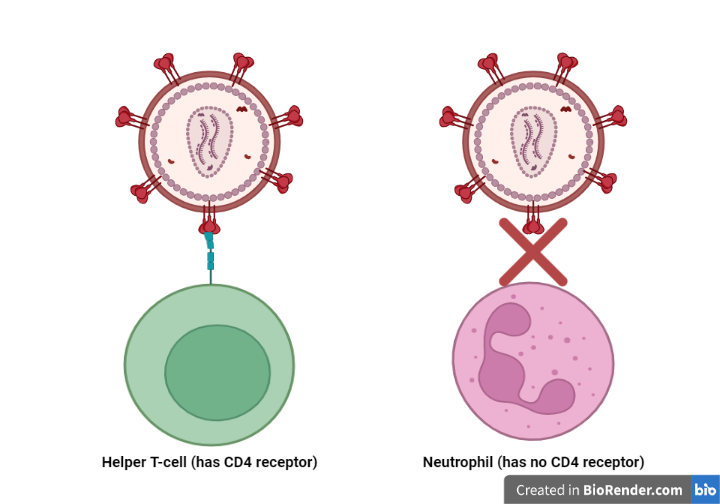
HIV infects a person by entering the bloodstream through a wound, unprotected sex, or from mother to child during pregnancy. HIV multiplies in the bloodstream by invading a specific group of immune cells called CD4-expressing T cells. These immune cells have spikes on their spherical surfaces called CD4 (Figure 1). The CD4 spikes act as hinges for HIV to latch onto. Once HIV grabs hold of these hinges, HIV fuses itself with its cellular victim. This fusion creates an opening for the virus to enter the immune cell3. Once HIV enters the immune cell, it hijacks the immune cell’s machinery. Instead of the immune cell maintaining itself, the virus forces its host to produce more HIV particles. The invaded immune cells then die, reducing the number of CD4 immune cells in the body. When doctors see that a person’s CD4 cell count falls below 200 cells/cubic mL of blood, they diagnose the person with AIDS.

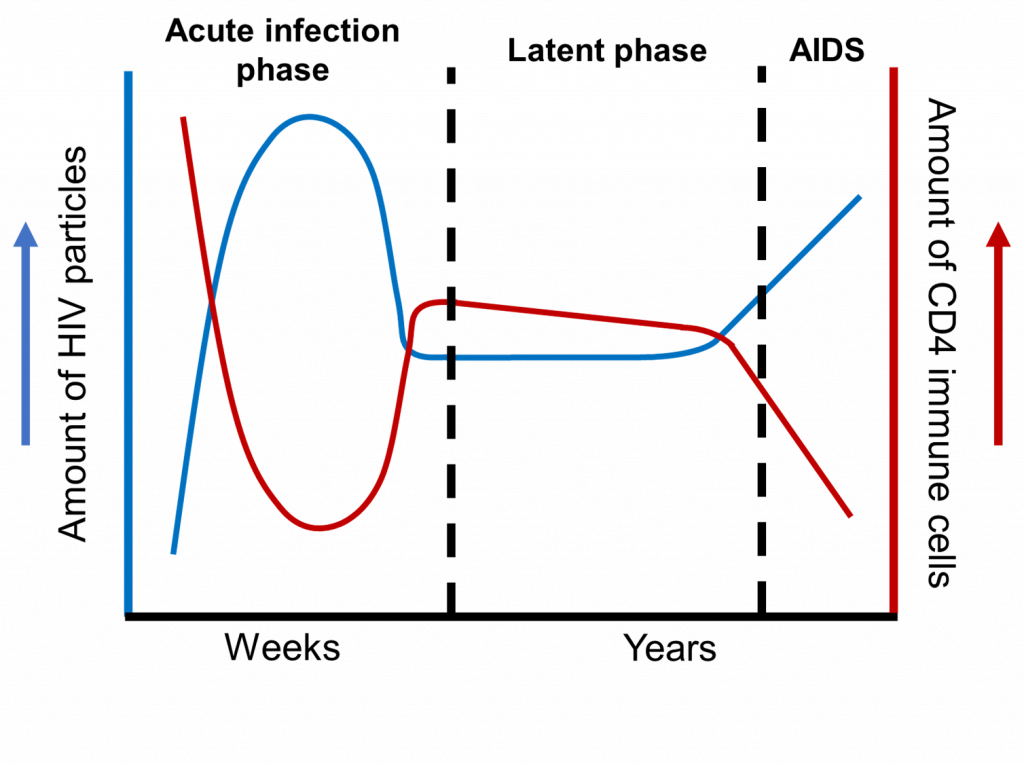
When HIV enters the bloodstream, the infected person will experience three stages (Figure 1)4. First, an HIV-infected person enters the acute infection stage, occurring 2-4 weeks after the first infection. During this phase, the number of HIV particles skyrockets and the CD4 cell count plummets. At the same time, a person will feel flu-like symptoms and have skin rashes all over their body. While the immune system can fight off the initial infection, surviving HIV populations remain in the body. These viruses lay dormant inside the immune cells they infected5. This dormancy characterizes the latent phase. The infected person can go on with life and have no idea that HIV remains in their body. After all, the infected person will not have any symptoms during the latent phase. The person may also have no idea that their CD4 counts are lower than usual because of the initial HIV infection. After about a decade, acquired immunodeficiency syndrome (AIDS) sets in. Just before a person has AIDS, the HIV populations reactivate. The reactivated virus kills more CD4 cells and weakens the immune system even more. The AIDS patient now has a severely compromised immune system. An AIDS patient would then be more likely to catch other infectious diseases like tuberculosis.

What happens to a person infected by HIV-B?
It’s already bad enough for a typical HIV variant to infect a person. If HIV treatment fails, a person will be more likely to have AIDS and die6. The new HIV variant compounds this problem. HIV-B causes AIDS in HIV-infected patients much more quickly. The CD4 cell counts among HIV-B infected patients are expected to reach below 200 cells/cubic mL of blood three times faster than patients infected by a non-HIV-B variant. Although HIV-B patients experience AIDS sooner, they thankfully have a similar 10-year survival rate as other HIV patients. The authors attribute this lack of difference to doctors treating HIV-B patients more quickly and intensely. Patients who do not have access to anti-HIV therapies, however, will face far greater danger if infected by HIV-B.
Variants among us: HIV and SARS-Cov-2
With all the talk of SARS-Cov-2 variants making the rounds, the discourse about HIV-B seems extremely relevant. Even though the two viruses cause disease in different ways, there are similarities between them. First, both viruses are positive-sense single-stranded RNA viruses. This means that RNA viruses can skip transcription and immediately produce proteins through translation (see this post to learn more about transcriptional and translation!). In doing so, RNA viruses can produce themselves far more quickly when activated. Both viruses can also mutate into new variants. SARS-Cov-2 has multiple variants like Omicron and its descendent BA.2. HIV has two major types: HIV-1 and HIV-2. HIV-1 is the predominant variant found worldwide, while HIV-2 is less common and mostly restricted to Western Africa8. HIV-1 also comprises variants, one of which is the newly discovered HIV-B variant.
About HIV-B
The HIV-B variant was first identified in a patient living in Amsterdam in 1992. The variant arose from the original HIV-1 type and has now developed over 500 mutations. Some of these mutations are also present in the 1992 isolate of the HIV-B variant. With some of the HIV-B mutations already present in the 1992 isolate, the earlier HIV isolates likely mutated to become HIV-B while infecting other patients. The over 500 mutations present in the HIV-B genomes are also spread out evenly. The even distribution of these mutations makes it harder to identify a specific gene mutation that makes HIV-B even more dangerous. As a comparison, the Omicron variant has over 32 mutations in the spike protein alone (see this post to learn more about Omicron!). Those mutations likely arose because SARS-Cov-2 has to bind to the ACE2 receptor with the spike protein to invade our lungs.
What next for HIV research?
The BEEHIVE study focuses a lot of effort on identifying the parts of the HIV genome that worsen infection outcomes. In the process, the UK-based scientists identified the HIV-B variant. It’s quite a find that lends itself to many more questions about HIV.
- How likely will HIV-B spread between patients? The authors claim that the rate of infections peaked in 2008. However, they also rightly note that it’s difficult to say for certain. It would be interesting to see whether HIV-B is only present in Europe or whether the virus has spread to other continents as well.
- Are there previously unrecognized mechanisms of infection caused only by HIV-B? The authors also identified a series of mutations that could help HIV-B escape destruction by white blood cells. They also identified a mutation to a protein that could cause even more T cell killing. While the authors identified mutations that could contribute to AIDS onset, it’s difficult to know for sure what role they play without more experiments.
- How effective are current treatments at treating HIV-B infections? It’s interesting to see that AIDS patients infected by HIV-B have a similar life expectancy as other HIV patients, even when HIV-B infections fasten AIDS onset. I think that being able to sample more patients and finding ways to monitor them and their treatments in clinical studies would help answer this question.
The emergence of HIV-B infections in the literature shows us that viruses can mutate to make disease worse. However, a lot more work needs to be done on how HIV-B makes infections worse and whether HIV-B can evade current treatment methods. The latter is especially important; failed treatment could increase the risk of death for AIDS patients infected by HIV-B. I also appreciate that the news of HIV-B emerged now. At a time where COVID-19 dominates news headlines and health responses, we have to remember to talk about and treat other diseases and viruses making people’s lives miserable.
References
- The BEEHIVE team. Oxford University. https://www.beehive.ox.ac.uk/
- Boender, T.S., Smit, C., Sighem, A. van, Bezemer, D., Ester, C.J., Zaheri, S., Wit, F.W.N.M., Reiss, P., and ATHENA national observational HIV cohort (2018). AIDS Therapy Evaluation in the Netherlands (ATHENA) national observational HIV cohort: cohort profile. BMJ Open 8, e022516.
- Wilen, C.B., Tilton, J.C., and Doms, R.W. (2012). HIV: Cell Binding and Entry. Cold Spring Harbor Perspectives in Medicine 2.
- Moir, S., Chun, T.-W., and Fauci, A.S. (2011). Pathogenic mechanisms of HIV disease. Annu Rev Pathol 6, 223–248.
- Siliciano, R.F., and Greene, W.C. (2011). HIV Latency. Cold Spring Harb Perspect Med 1, a007096.
- Grabar, S., Le Moing, V., Goujard, C., Leport, C., Kazatchkine, M.D., Costagliola, D., and Weiss, L. (2000). Clinical outcome of patients with HIV-1 infection according to immunologic and virologic response after 6 months of highly active antiretroviral therapy. Ann Intern Med 133, 401–410.
- Bbosa, N., Kaleebu, P., and Ssemwanga, D. (2019). HIV subtype diversity worldwide. Curr Opin HIV AIDS 14, 153–160.

